{{Lead missing|date=January 2026}}
{{Infobox medical condition (new)
{{Infobox medical condition (new)
| name =
| name =
| deaths =
| deaths =
}}
}}
”’Right atrial enlargement”’ (RAE) is a form of [[cardiomegaly]], or heart enlargement. It can broadly be classified as either right atrial hypertrophy (RAH), overgrowth, or dilation, like an expanding balloon. Right atrial enlargement (RAE) is clinically significant due to its prevalence in diagnosing supraventricular arrhythmias.
”’Right atrial enlargement”’ (RAE) is a form of [[cardiomegaly]], or heart enlargement. It can broadly be classified as either right atrial hypertrophy (RAH), overgrowth, or dilation, like an expanding balloon. Common causes include [[pulmonary hypertension]], which can be the primary defect leading to RAE, or pulmonary hypertension secondary to [[tricuspid stenosis]]; [[pulmonary stenosis]] or [[Tetralogy of Fallot]] i.e. congenital diseases; chronic lung disease, such as [[cor pulmonale]]. Other recognised causes are: [[right ventricular failure]], [[tricuspid regurgitation]], and [[atrial septal defect]].<ref>{{cite web |url=https://123sonography.com/ebook/size-of-right-atrium-and-associated-structures |title=Size of the right atrium and associated structures |author=<!–Staff writer(s); no by-line.–> |date= 2012-08-20|website=123 sonography.com |publisher=Medical University of Vienna |access-date=13 December 2016}}</ref> Right atrial enlargement (RAE) is clinically significant due to its prevalence in diagnosing supraventricular arrhythmias. Further, early diagnosis using risk factors like RAE may decrease mortality because patients with RAE are at 9x more risk of arrhythmias and other cardiac conditions compared to their healthy counterparts.<ref name=”Ho Low Zhang Le 2018 pp. 237–242″>{{cite journal | last1=Ho | first1=A.K. | last2=Low | first2=G. | last3=Zhang | first3=Yi | last4=Le | first4=Lawrence H. | last5=Minosse | first5=Silvia | last6=Vidiri | first6=Antonello | last7=Zheng | first7=Rui | last8=Lou | first8=Edmond | last9=Edam | first9=A.N. | last10=Bradley | first10=D.A. | last11=Nguyen | first11=Vu-Hieu | last12=Le | first12=Lawrence H. | title=Right atrium enlargement predicts clinically significant supraventricular arrhythmia in patients with pulmonary arterial hypertension | journal=Heart & Lung | publisher=Mosby | volume=47 | issue=3 | date=May 1, 2018 | issn=0147-9563 | doi=10.1016/j.hrtlng.2018.01.004 | pages=237–242 | s2cid=3363049 |url=https://www.sciencedirect.com/science/article/abs/pii/S0147956317302169 | access-date=December 29, 2023| url-access=subscription }}</ref> Treatment for RAE can include taking certain medications such as diuretics, beta-blockers, anticoagulants, and anti-arrhythmics. If medications are not effective enough, procedures such as implanting a pacemaker, cardioverter-defibrillator (ICD), or a left ventricular assist device (LVAD), heart valve surgery, and coronary bypass surgery may be needed.<ref name=”w944″>{{cite journal | last1=Surace | first1=Francesca Chiara | last2=Iezzi | first2=Federica | last3=Colaneri | first3=Massimo | last4=Pozzi | first4=Marco | title=Surgical Treatment of Idiopathic Enlargement of the Right Atrium | journal=Case Reports in Surgery | publisher=Hindawi Limited | volume=2018 | date=2018-09-20 | issn=2090-6900 | doi=10.1155/2018/7241309 | doi-access=free | pages=1–5| pmc=6171214 }}</ref> The last resort treatment option would be a complete heart transplant. Prevention for RAE comes from maintaining a healthy lifestyle with plenty of exercise and eating plenty of vegetables, fruits, and whole grains and avoiding or limiting alcohol and caffeine.<ref name=”n153″>{{cite web | title=Enlarged heart-Enlarged heart | website=Mayo Clinic | date=2022-05-04 | url=https://www.mayoclinic.org/diseases-conditions/enlarged-heart/diagnosis-treatment/drc-20355442#self-care | access-date=2024-11-22}}</ref> It is also important to control heart disease risk factors including diabetes, high cholesterol, and high blood pressure. Exercise, pregnancy, and prior health conditions like ASD II can also promote cardiac remodeling, so routine primary care visits are important to distinguish between physiological and pathological atrial enlargement.<ref name=”d449″>{{cite journal | last1=Chen | first1=Yi Ching | last2=Voskoboinik | first2=Aleksandr | last3=Gerche | first3=Andre La | last4=Marwick | first4=Thomas H. | last5=McMullen | first5=Julie R. | title=Prevention of Pathological Atrial Remodeling and Atrial Fibrillation | journal=Journal of the American College of Cardiology | volume=77 | issue=22 | date=2021 | doi=10.1016/j.jacc.2021.04.012 | doi-access=free | pages=2846–2864}}</ref><ref name=”m482″>{{cite journal | last1=W | first1=Piesiewicz | last2=A | first2=Goch | last3=Z | first3=Binikowski | last4=U | first4=Faflik | last5=G | first5=Krasomski | last6=JH | first6=Goch | title=Changes in the cardiovascular system during pregnancy in women with secondary atrial septal defect | journal=Kardiologia Polska | publisher=Kardiol Pol | volume=60 | issue=3 | issn=0022-9032 | pmid=15156217 | page=}}</ref> Regular primary care visits and routine testing has also been shown to protect against the development of cardiovascular disease and may play a key role in early identification and treatment.<ref name=”v883″>{{cite journal | last1=Einarsdóttir | first1=Kristjana | last2=Preen | first2=David B. | last3=Emery | first3=Jon D. | last4=Holman | first4=C. D’Arcy J. | title=Regular Primary Care Plays a Significant Role in Secondary Prevention of Ischemic Heart Disease in a Western Australian Cohort | journal=Journal of General Internal Medicine | publisher=Springer Science and Business Media LLC | volume=26 | issue=10 | date=2011-02-24 | issn=0884-8734 | doi=10.1007/s11606-011-1665-1 | doi-access=free | pages=1092–1097| pmc=3181311 }}</ref>
==Signs and symptoms==
==Signs and symptoms==
==Causes==
==Causes==
Common causes include [[pulmonary hypertension]], which can be the primary defect leading to RAE, or pulmonary hypertension secondary to [[tricuspid stenosis]]; [[pulmonary stenosis]] or [[Tetralogy of Fallot]] i.e. congenital diseases; chronic lung disease, such as [[cor pulmonale]]. Other recognised causes are: [[right ventricular failure]], [[tricuspid regurgitation]], and [[atrial septal defect]].<ref>{{cite web |url=https://123sonography.com/ebook/size-of-right-atrium-and-associated-structures |title=Size of the right atrium and associated structures |author=<!–Staff writer(s); no by-line.–> |date= 2012-08-20|website=123 sonography.com |publisher=Medical University of Vienna |access-date=13 December 2016}}</ref>
Most authors have classified this condition as congenital, but the etiology is still unknown.<ref name=”Terada Oiwake Nakanuma Ohta 1988 pp. 361–370″/>
Most authors have classified this condition as congenital, but the etiology is still unknown.<ref name=”Terada Oiwake Nakanuma Ohta 1988 pp. 361–370″/>
Large “a” waves on the [[Jugular venous pressure|JVP waveform]] can also aid in diagnosis.
Large “a” waves on the [[Jugular venous pressure|JVP waveform]] can also aid in diagnosis.
Early diagnosis using risk factors like RAE may decrease mortality because patients with RAE are at 9x more risk of arrhythmias and other cardiac conditions compared to their healthy counterparts.<ref name=”Ho Low Zhang Le 2018 pp. 237–242″>{{cite journal | last1=Ho | first1=A.K. | last2=Low | first2=G. | last3=Zhang | first3=Yi | last4=Le | first4=Lawrence H. | last5=Minosse | first5=Silvia | last6=Vidiri | first6=Antonello | last7=Zheng | first7=Rui | last8=Lou | first8=Edmond | last9=Edam | first9=A.N. | last10=Bradley | first10=D.A. | last11=Nguyen | first11=Vu-Hieu | last12=Le | first12=Lawrence H. | title=Right atrium enlargement predicts clinically significant supraventricular arrhythmia in patients with pulmonary arterial hypertension | journal=Heart & Lung | publisher=Mosby | volume=47 | issue=3 | date=May 1, 2018 | issn=0147-9563 | doi=10.1016/j.hrtlng.2018.01.004 | pages=237–242 | s2cid=3363049 |url=https://www.sciencedirect.com/science/article/abs/pii/S0147956317302169 | access-date=December 29, 2023| url-access=subscription }}</ref>
==Treatment==
Treatment for RAE can include taking certain medications such as diuretics, beta-blockers, anticoagulants, and anti-arrhythmics. If medications are not effective enough, procedures such as implanting a pacemaker, cardioverter-defibrillator (ICD), or a left ventricular assist device (LVAD), heart valve surgery, and coronary bypass surgery may be needed.<ref name=”w944″>{{cite journal | last1=Surace | first1=Francesca Chiara | last2=Iezzi | first2=Federica | last3=Colaneri | first3=Massimo | last4=Pozzi | first4=Marco | title=Surgical Treatment of Idiopathic Enlargement of the Right Atrium | journal=Case Reports in Surgery | publisher=Hindawi Limited | volume=2018 | date=2018-09-20 | issn=2090-6900 | doi=10.1155/2018/7241309 | doi-access=free | pages=1–5| pmc=6171214 }}</ref> The last resort treatment option would be a complete heart transplant.
==Prevention==
Prevention for RAE comes from maintaining a healthy lifestyle with plenty of exercise and eating plenty of vegetables, fruits, and whole grains and avoiding or limiting alcohol and caffeine.<ref name=”n153″>{{cite web | title=Enlarged heart-Enlarged heart | website=Mayo Clinic | date=2022-05-04 | url=https://www.mayoclinic.org/diseases-conditions/enlarged-heart/diagnosis-treatment/drc-20355442#self-care | access-date=2024-11-22}}</ref> It is also important to control heart disease risk factors including diabetes, high cholesterol, and high blood pressure. Exercise, pregnancy, and prior health conditions like ASD II can also promote cardiac remodeling, so routine primary care visits are important to distinguish between physiological and pathological atrial enlargement.<ref name=”d449″>{{cite journal | last1=Chen | first1=Yi Ching | last2=Voskoboinik | first2=Aleksandr | last3=Gerche | first3=Andre La | last4=Marwick | first4=Thomas H. | last5=McMullen | first5=Julie R. | title=Prevention of Pathological Atrial Remodeling and Atrial Fibrillation | journal=Journal of the American College of Cardiology | volume=77 | issue=22 | date=2021 | doi=10.1016/j.jacc.2021.04.012 | doi-access=free | pages=2846–2864}}</ref><ref name=”m482″>{{cite journal | last1=W | first1=Piesiewicz | last2=A | first2=Goch | last3=Z | first3=Binikowski | last4=U | first4=Faflik | last5=G | first5=Krasomski | last6=JH | first6=Goch | title=Changes in the cardiovascular system during pregnancy in women with secondary atrial septal defect | journal=Kardiologia Polska | publisher=Kardiol Pol | volume=60 | issue=3 | issn=0022-9032 | pmid=15156217 | page=}}</ref>
Regular primary care visits and routine testing has also been shown to protect against the development of cardiovascular disease and may play a key role in early identification and treatment.<ref name=”v883″>{{cite journal | last1=Einarsdóttir | first1=Kristjana | last2=Preen | first2=David B. | last3=Emery | first3=Jon D. | last4=Holman | first4=C. D’Arcy J. | title=Regular Primary Care Plays a Significant Role in Secondary Prevention of Ischemic Heart Disease in a Western Australian Cohort | journal=Journal of General Internal Medicine | publisher=Springer Science and Business Media LLC | volume=26 | issue=10 | date=2011-02-24 | issn=0884-8734 | doi=10.1007/s11606-011-1665-1 | doi-access=free | pages=1092–1097| pmc=3181311 }}</ref>
==See also==
==See also==
Medical condition
Right atrial enlargement (RAE) is a form of cardiomegaly, or heart enlargement. It can broadly be classified as either right atrial hypertrophy (RAH), overgrowth, or dilation, like an expanding balloon. Right atrial enlargement (RAE) is clinically significant due to its prevalence in diagnosing supraventricular arrhythmias.
Symptoms of right atrial enlargement include palpitations, dyspnea, paroxysmal tachycardia, general malaise, shortness of breath, syncope, chest pain, fatigue, cyanosis, loss of appetite, tachycardia, fever, and cough. Many patients with right atrial enlargement are asymptomatic.[1]
Common causes include pulmonary hypertension, which can be the primary defect leading to RAE, or pulmonary hypertension secondary to tricuspid stenosis; pulmonary stenosis or Tetralogy of Fallot i.e. congenital diseases; chronic lung disease, such as cor pulmonale. Other recognised causes are: right ventricular failure, tricuspid regurgitation, and atrial septal defect.[2]
Most authors have classified this condition as congenital, but the etiology is still unknown.[1]
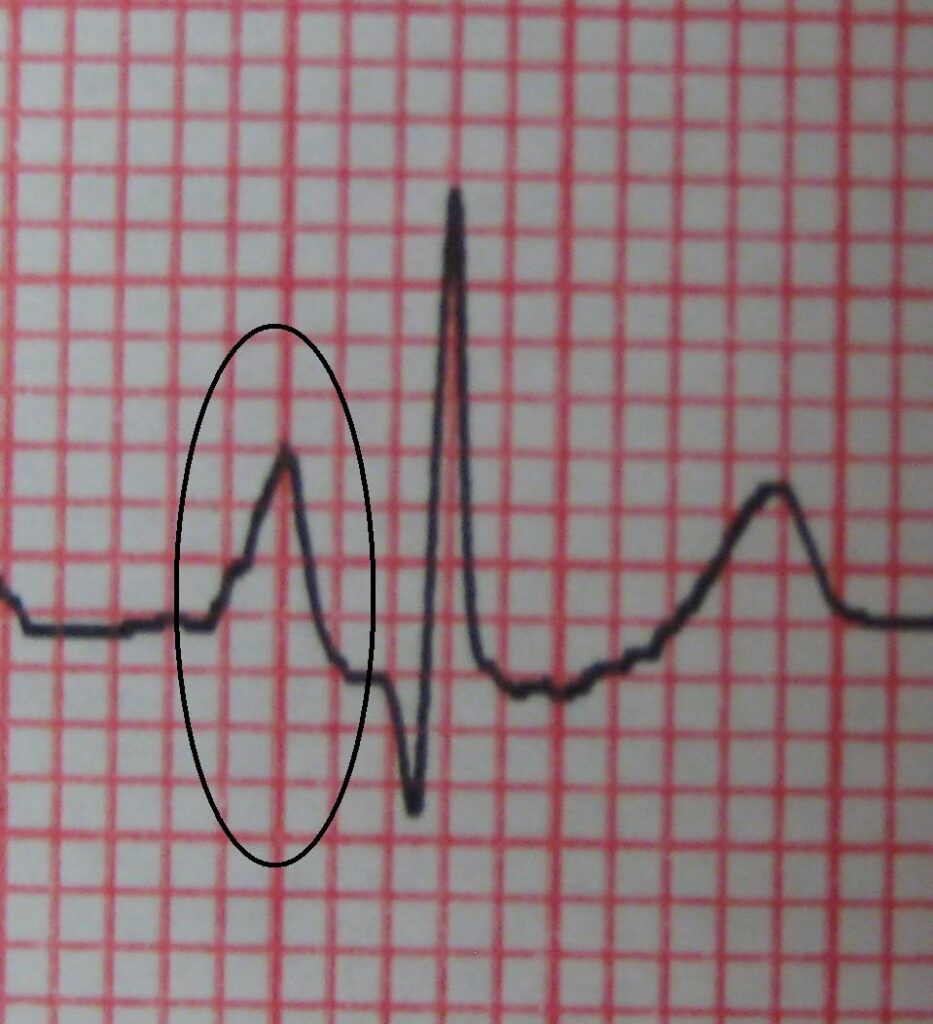
Right Atrial Enlargement (RAE) increases the p wave, representing atrial depolarization, on an ECG to an amplitude > 2.5mm in lead II, an abnormality referred to as p-pulmonale, likely due to weakened right atrial myocardium close to the Sinoatrial (SA) node.[3]
ECG criteria for RAE: P wave amplitude in lead II > 2.5 mm and upward deflection of the P wave in lead V1 > 1.5 mm in amplitude.[4]
Large “a” waves on the JVP waveform can also aid in diagnosis.
Early diagnosis using risk factors like RAE may decrease mortality because patients with RAE are at 9x more risk of arrhythmias and other cardiac conditions compared to their healthy counterparts.[5]
Treatment for RAE can include taking certain medications such as diuretics, beta-blockers, anticoagulants, and anti-arrhythmics. If medications are not effective enough, procedures such as implanting a pacemaker, cardioverter-defibrillator (ICD), or a left ventricular assist device (LVAD), heart valve surgery, and coronary bypass surgery may be needed.[6] The last resort treatment option would be a complete heart transplant.
Prevention for RAE comes from maintaining a healthy lifestyle with plenty of exercise and eating plenty of vegetables, fruits, and whole grains and avoiding or limiting alcohol and caffeine.[7] It is also important to control heart disease risk factors including diabetes, high cholesterol, and high blood pressure. Exercise, pregnancy, and prior health conditions like ASD II can also promote cardiac remodeling, so routine primary care visits are important to distinguish between physiological and pathological atrial enlargement.[8][9]
Regular primary care visits and routine testing has also been shown to protect against the development of cardiovascular disease and may play a key role in early identification and treatment.[10]
- ^ a b Terada, Tadashi; Oiwake, Hisanori; Nakanuma, Yasuni; Ohta, Goroku; Nishino, Tomoichi (1988). “An Autopsy Case of Idiopathic Enlargement of the Right Atrium, and a Review of the Literature”. Pathology International. 38 (3): 361–370. doi:10.1111/j.1440-1827.1988.tb02308.x. ISSN 1320-5463. PMID 2969171. S2CID 41759734.
- ^ “Size of the right atrium and associated structures”. 123 sonography.com. Medical University of Vienna. 2012-08-20. Retrieved 13 December 2016.
- ^ G, Limongelli; D, Masarone; G, Frisso; M, Iacomino; I, Ferrara; A, Rea; R, Gravino; E, Bossone; F, Salvatore; R, Calabro; P, Elliott; G, Pacileo (2017). “Clinical and genetic characterization of patients with hypertrophic cardiomyopathy and right atrial enlargement”. Journal of Cardiovascular Medicine (Hagerstown, Md.). 18 (4). J Cardiovasc Med (Hagerstown): 249–254. doi:10.2459/JCM.0000000000000361. ISSN 1558-2035. PMID 26808413. S2CID 25505222.
- ^ Surawicz, Borys; Childers, Rory; Deal, Barbara J.; Gettes, Leonard S. (2009). “AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram”. Circulation. 119 (10): e235-40. doi:10.1161/circulationaha.108.191095. PMID 19228822. S2CID 26702140.
- ^ Ho, A.K.; Low, G.; Zhang, Yi; Le, Lawrence H.; Minosse, Silvia; Vidiri, Antonello; Zheng, Rui; Lou, Edmond; Edam, A.N.; Bradley, D.A.; Nguyen, Vu-Hieu; Le, Lawrence H. (May 1, 2018). “Right atrium enlargement predicts clinically significant supraventricular arrhythmia in patients with pulmonary arterial hypertension”. Heart & Lung. 47 (3). Mosby: 237–242. doi:10.1016/j.hrtlng.2018.01.004. ISSN 0147-9563. S2CID 3363049. Retrieved December 29, 2023.
- ^ Surace, Francesca Chiara; Iezzi, Federica; Colaneri, Massimo; Pozzi, Marco (2018-09-20). “Surgical Treatment of Idiopathic Enlargement of the Right Atrium”. Case Reports in Surgery. 2018. Hindawi Limited: 1–5. doi:10.1155/2018/7241309. ISSN 2090-6900. PMC 6171214.
- ^ “Enlarged heart-Enlarged heart”. Mayo Clinic. 2022-05-04. Retrieved 2024-11-22.
- ^ Chen, Yi Ching; Voskoboinik, Aleksandr; Gerche, Andre La; Marwick, Thomas H.; McMullen, Julie R. (2021). “Prevention of Pathological Atrial Remodeling and Atrial Fibrillation”. Journal of the American College of Cardiology. 77 (22): 2846–2864. doi:10.1016/j.jacc.2021.04.012.
- ^ W, Piesiewicz; A, Goch; Z, Binikowski; U, Faflik; G, Krasomski; JH, Goch. “Changes in the cardiovascular system during pregnancy in women with secondary atrial septal defect”. Kardiologia Polska. 60 (3). Kardiol Pol. ISSN 0022-9032. PMID 15156217.
- ^ Einarsdóttir, Kristjana; Preen, David B.; Emery, Jon D.; Holman, C. D’Arcy J. (2011-02-24). “Regular Primary Care Plays a Significant Role in Secondary Prevention of Ischemic Heart Disease in a Western Australian Cohort”. Journal of General Internal Medicine. 26 (10). Springer Science and Business Media LLC: 1092–1097. doi:10.1007/s11606-011-1665-1. ISSN 0884-8734. PMC 3181311.
- J, Zhang; L, Zhang; L, He; H, Li; Y, Li; L, Zhang; M, Xie (2021). “Clinical Presentation, Diagnosis, and Management of Idiopathic Enlargement of the Right Atrium: An Analysis Based on Systematic Review of 153 Reported Cases”. Cardiology. 146 (1): 88–97. doi:10.1159/000511434. ISSN 1421-9751. PMID 33242857.
- Hughes, William E.; Casey, Darren P.; Baldini, Francesca; Vergani, Laura; Guo, Junxia; Fan, Zhenping; Wang, Zhenwei; Liu, Nai-Feng; Motoki, Hirohiko; Klein, Allan L.; Tandaju, Jeremy R.; Raeisi-Dehkordi, Hamidreza (February 1, 2022). “Right atrium enlargement is related to increased heart damage and mortality in well-controlled hypertension”. Nutrition, Metabolism and Cardiovascular Diseases. 32 (2). Elsevier: 420–428. doi:10.1016/j.numecd.2021.10.004. ISSN 0939-4753. PMID 34893418. Retrieved December 29, 2023.