== Clinical Impacts ==
== Clinical Impacts ==
There was a heavy [[hospital]] burden in Peshawar with five main hospitals reporting the documented cases.<ref name=”:5″ /> Patients from these hospitals were moved between endemic and non-endemic areas which amplified the initial outbreak.<ref>{{Cite journal |last=Shah |first=Fahad |last2=Butt |first2=Maryam |last3=Iqbal |first3=Attiya |last4=Shah |first4=Mian Naveed |last5=Muhammad |first5=Lal |last6=Kousar |first6=Nasim |last7=Ulhaq |first7=Farid |date=2018 |title=Institutional analysis of 2017 dengue outbreaks of Peshawar, Khyber Pakhtoonkhwa, Pakistan |url=https://www.researchgate.net/publication/325113041_Institutional_analysis_of_2017_dengue_outbreaks_of_Peshawar_Khyber_Pakhtoonkhwa_Pakistan |journal=Journal of Entomology and Zoology Studies |volume=6 |issue=2 |pages=2475-2479 |eissn=2320-7078 |via=Entomol Journal}}</ref> There was a loss of work days in young adults (16-30 years) who were the most affected group leading to local [[economic]] impacts.<ref name=”:5″ /> There were reports of fever, body [[Ache|aches]], [[vomiting]], [[Rash|skin rashes]], [[Gum bleeding|gum]] [[Gum bleeding|bleeding]], [[Nosebleed|nosebleeds]] and [[elevated liver enzymes]].<ref name=”:5″ /><ref name=”:7″ /> Fevers were universal but [[headache]], [[fatigue]] and [[Hepatomegaly|liver enlargement]] were highly prevalent.<ref name=”:7″ /> [[IgM antibodies]] were detected in 180 cases that confirmed both [[Primary infection|primary]] and [[Secondary infection|secondary infections]].<ref name=”:7″ /> Most cases were identified as dengue fever and few progressed to [[dengue hemorrhagic fever]] and there was no [[dengue shock syndrome]] reported.<ref name=”:7″ /> The [[case fatality rate]] was 0.28% which was lower than the previous epidemics in Lahore and Swat.<ref name=”:5″ />
There was a heavy [[hospital]] burden in Peshawar with five main hospitals reporting the documented cases.<ref name=”:5″ /> Patients from these hospitals were moved between endemic and non-endemic areas which amplified the initial outbreak.<ref>{{Cite journal |last=Shah |first=Fahad |last2=Butt |first2=Maryam |last3=Iqbal |first3=Attiya |last4=Shah |first4=Mian Naveed |last5=Muhammad |first5=Lal |last6=Kousar |first6=Nasim |last7=Ulhaq |first7=Farid |date=2018 |title=Institutional analysis of 2017 dengue outbreaks of Peshawar, Khyber Pakhtoonkhwa, Pakistan |url=https://www.researchgate.net/publication/325113041_Institutional_analysis_of_2017_dengue_outbreaks_of_Peshawar_Khyber_Pakhtoonkhwa_Pakistan |journal=Journal of Entomology and Zoology Studies |volume=6 |issue=2 |pages=2475-2479 |eissn=2320-7078 |via=Entomol Journal}}</ref> There was a loss of work days in young adults (16-30 years) who were the most affected group leading to local [[economic]] impacts.<ref name=”:5″ /> There were reports of fever, body [[Ache|aches]], [[vomiting]], [[Rash|skin rashes]], [[Gum bleeding|gum]] [[Gum bleeding|bleeding]], [[Nosebleed|nosebleeds]] and [[elevated liver enzymes]].<ref name=”:5″ /><ref name=”:7″ /> Fevers were universal but [[headache]], [[fatigue]] and [[Hepatomegaly|liver enlargement]] were highly prevalent.<ref name=”:7″ /> [[IgM antibodies]] were detected in 180 cases that confirmed both [[Primary infection|primary]] and [[Secondary infection|secondary infections]].<ref name=”:7″ /> Most cases were identified as dengue fever and few progressed to [[dengue hemorrhagic fever]] and there was no [[dengue shock syndrome]] reported.<ref name=”:7″ /> The [[case fatality rate]] was 0.28% which was lower than the previous epidemics in Lahore and Swat.<ref name=”:5″ />
== Health Consequences of Dengue Fever ==
== Health Consequences of Dengue Fever ==
=== Public Health Impact ===
=== Public Health Impact ===
Beyond individual health, dengue outbreaks like the one in Peshawar have significant social and economic consequences. High infection rates strain healthcare systems, increase hospital admissions, and disrupt daily life due to widespread illness and fear of infection. Long-term recovery periods and recurring outbreaks can reduce workforce productivity and create financial hardship, especially in low-income communities.
Beyond individual health, dengue outbreaks like the one in Peshawar have significant social and economic consequences. High infection rates strain healthcare systems, increase hospital admissions, and disrupt daily life due to widespread illness and fear of infection. Long-term recovery periods and recurring outbreaks can reduce workforce productivity and create financial hardship, especially in low-income communities.
== Lessons learned ==
== Lessons learned ==

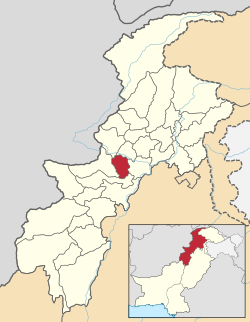
Peshawar is the sixth largest city in Pakistan with a total area of 1,257 square kilometres, it is the capital of the Khyber Pakhtunkhwa province in Northern Pakistan. It is located on the flat Gandhara Plains, surrounded by mountain ranges on three sides. The climate is generally warm with an average temperature of 22.3 degrees Celsius and rainfall throughout the year. [1]
The estimated population of Peshawar is 2.5 million, growing exponentially from 500,000 in 1980.[2] The average household size in 2017 was 7.97 with a known housing shortage. Pashtuns are the main ethnic group, though Peshawar has seen a large influx of Afghans resulting in unplanned and haphazard growth which governmental initiatives did not account for, resulting in ad-hoc planning and development and massive urban-sprawl which infrastructure, institutions and civic services struggle to support, particularly in the slum and settlement areas where poverty is high. [3] Water supply and drainage systems in these areas are poor, resulting in increased water stagnation, especially in flooding seasons. [3]
Dengue is a non-contagious single-stranded positive-sense RNA viral infection, found in over 125 countries annually, spread by mosquitoes carrying the epidemic vectors Aedes Albopictus and Aedes Aegypti. It belongs to the family Flaviviridae, the genus Flavivirus and has five strains. These mosquitoes are most often found in urban indoor environments during daytime.[4]
The World Health Organisation (WHO) considers dengue part of the top ten global health issues, with over 100 million cases resulting in 20,000-25,000 deaths annually, making it the leading cause of arthropod-born viral disease worldwide. It has an incubation phase of four to seven days, with symptoms lasting three to ten days.[4] There is no cure and treatment involves managing symptoms.[1]
Total dengue cases are often underestimated as over 50% of those infected are either; asymptomatic, have mild flu-like symptoms which they self-manage or are misdiagnosed.[5] Up to 5% of cases develop severe symptoms resulting in shock, organ failure, haemorrhage and potentially death. The severity of symptoms is influenced by various host, environmental and virus factors.[4]
A positive association exists between rainfall, temperature and humidity, and dengue fever prevalence.[6] With prevalence highest in tropical and subtropical environments across the Americas, Asia and Africa.[5] Pakistan has had ten major outbreaks since 1982.[1]
Details Of The Disaster
[edit]
Throughout 2017 the Ministry of National Health Services, Regulations and Coordination in Pakistan reported higher than usual numbers of dengue fever cases. The highest number of confirmed laboratory cases was 24,807 in the Khyber Pakhtunkhwa province resulting in 69 deaths by November 2017.[7] Of these, 23,541 confirmed cases with 65 deaths occurred in Peshawar, with most cases occurring in September (32%) and October (41%) during monsoon season.[8]
Between July to August 2017, 52% of those infected were aged 25-64 years old, 29% were 15-24, 15% were 0-14 years old and 3% were over 65. 62% of those infected were male.[7]
Pakistan has experienced nearly annual dengue epidemics with previous notable outbreaks in Lahore and Swat. Dengue was already endemic across much of Pakistan by July 2017.[5]
| Month | Event |
|---|---|
| July | A dengue situation was declared in Khyber Pakhtunkhwa province with over 500 positive cases.[9] |
| August | Pakistan Red Crescent Society (PRCS) began initial screening camps and awareness drives in high-risk areas using provincial resources.[9] |
| September | National authorities confirmed the outbreak as an emergency dengue disaster with 75,000 suspected cases, 24,382 confirmed, 73 deaths mainly in Peshawar.[9] |
| October | October had the highest number of cases which coincided with the end of the monsoon rains. Vector surveillance with WHO identified “hot-spots” and started intensive community interventions. [8] |
| October-November | Six new screening/diagnostic camps established (esp. Peshawar City, Nowshera, Mansehra). Mass school and community awareness campaigns conducted.[9] |
| November | Rapid decline in dengue cases.[9] |
Spatial distribution of the Dengue outbreak
[edit]
The dengue outbreak affected 15 districts in Khyber Pakhtunkhwa province with Peshawar at the epicentre, diffused throughout the region by the Aedes aegypti mosquito.[8] Urbanisation and improved travel infrastructure allowed the migration of infected vectors and people between different districts. [10] The virus spread along key transport corridors to Mardan, Nowshera, Mansehra, Kohat, and Buner/Swabi.[9] There were smaller outbreaks in Abbotabad and Mardan due to high urban concentration of risk.[9] Rural areas had lower number of incidences but this could be due to potential under-reporting.[9] The outbreak unfolded over six months, peaking in August to early September 2017, in alignment with the regional monsoon season that promotes Aedes aegypti breeding.[11] The dense housing, standing water and poor drainage in these urban areas created stagnant water for ideal breeding sites for the mosquitos.[10] The seasonality of the monsoon, alongside the temperate climate and rain-fed agriculture explained the surge of cases in October.[10] Environmental mis-management and poor sanitation underpinned the spatial pattern.[9]
There was a heavy hospital burden in Peshawar with five main hospitals reporting the documented cases.[8] Patients from these hospitals were moved between endemic and non-endemic areas which amplified the initial outbreak.[12] There was a loss of work days in young adults (16-30 years) who were the most affected group leading to local economic impacts.[8] There were reports of fever, body aches, vomiting, skin rashes, gum bleeding, nosebleeds and elevated liver enzymes.[8][10] Fevers were universal but headache, fatigue and liver enlargement were highly prevalent.[10] IgM antibodies were detected in 180 cases that confirmed both primary and secondary infections.[10] Most cases were identified as dengue fever and few progressed to dengue hemorrhagic fever and there was no dengue shock syndrome reported.[10] The case fatality rate was 0.28% which was lower than the previous epidemics in Lahore and Swat.[8]
Health Consequences of Dengue Fever
[edit]
Short-term Health Consequences
[edit]
In Peshawar, 23,541 residents were laboratory-confirmed to have been infected with dengue fever. When underreporting and asymptomatic cases are taken into account, the actual number of infections is estimated to be considerably higher, indicating that tens of thousands of individuals suffered direct health impacts from the virus within a short period. The outbreak resulted in the deaths of 65 residents in Peshawar, representing an irreversible loss of life.[8]
The most common short-term health impacts typically began with a mild to high fever, which was experienced by nearly all patients (100%). [4]Severe headache, along with intense muscle and joint pain–characteristic symptoms of dengue fever–were also highly prevalent (95%), often causing significant discomfort and limiting patients’ ability to carry out normal activities. Nausea and vomiting occurred in a considerable number of patients (70%), potentially leading to dehydration and electrolyte imbalance. A rash appeared in nearly one-third of cases (30%). In the most severe instances (5%), patients exhibited bleeding tendencies and faced life-threatening complications such as shock and organ failure.[5]
The average age of dengue patients was approximately 26 years, with the majority of cases concentrated among individuals aged 16 to 30. This demographic represents a crucial segment of the social labor force, and their collective infection negatively impacted household livelihoods and posed challenges to social stability. Males faced a higher risk of infection (65.3%) and demonstrated a significantly greater likelihood of developing severe cases compared to females (accounting for 88.6% of fatal outcomes). This resulted in numerous families losing husbands, fathers, or sons, dealing a severe blow to family structures.[8]
Long-Term Health Consequences
[edit]
While most individuals recover completely within two weeks, some may experience long-lasting effects after the acute phase of infection. These post-dengue complications are sometimes referred to as post-dengue fatigue syndrome or post-viral syndrome, and may persist for weeks or even months after recovery. Common long-term symptoms include:
- Persistent fatigue and weakness
- Joint and muscle pain
- Difficulty concentrating or “brain fog”
- Mood changes, such as irritability or depression
- Reduced appetite and gradual weight loss
In rare cases, severe dengue can result in long-term organ damage. Liver inflammation (hepatitis), myocarditis (inflammation of the heart muscle), and neurological complications such as encephalitis, meningitis, or Guillain-Barré syndrome have been reported. These conditions can have lasting impacts on the patient’s quality of life and require prolonged medical care.
Repeated dengue infections, caused by different virus serotypes (DENV-1 to DENV-4), can also increase the risk of severe disease due to a phenomenon known as antibody-dependent enhancement (ADE). This occurs when antibodies from a previous dengue infection facilitate entry of a new serotype into host cells, leading to a stronger immune reaction and more severe illness during subsequent infections.
Public Health Impact
[edit]
Beyond individual health, dengue outbreaks like the one in Peshawar have significant social and economic consequences. High infection rates strain healthcare systems, increase hospital admissions, and disrupt daily life due to widespread illness and fear of infection. Long-term recovery periods and recurring outbreaks can reduce workforce productivity and create financial hardship, especially in low-income communities.
After the first dengue cases were confirmed in July 2017, the provincial government of Khyber Pakhtunkhwa (KP) launched an emergency public health response to contain the outbreak in Peshawar. With technical support from the World Health Organization (WHO), the provincial health department established a Dengue Response Unit to coordinate vector control, patient management, and surveillance activities.[13]
Health teams conducted door-to-door insecticide spraying, larvicidal treatment, and fumigation in high-risk neighborhoods. By October 2017, more than 190,000 households had been reached through these operations.[14]
Public awareness campaigns were organised in schools, mosques, and community centres. Residents were encouraged to remove standing water, use mosquito nets, and apply repellents to prevent bites. Hospitals and laboratories were strengthened to improve case detection and patient care.[13] The Pakistan Red Crescent Society (PRCS) deployed volunteers and mobile health camps that distributed mosquito nets and repellents, provided health education, and referred severe cases to hospitals.[15]
By the end of the outbreak, official reports estimated around 24,800 confirmed cases and about 70 deaths in KP province.[14] The combined interventions of local authorities, communities, and aid organisations helped reduce transmission and improve preparedness for future dengue epidemics.[13]
International response
[edit]
The WHO provided continuous technical and operational support to Khyber Pakhtunkhwa’s health authorities. WHO teams trained local health workers, monitored mosquito breeding sites, and improved data management systems.[13] The organisation identified Peshawar as the epicentre of the outbreak, reporting approximately 87,000 suspected cases, 18,900 confirmed infections, and 58 deaths.[13]
The IFRC supported PRCS operations in Khyber Pakhtunkhwa with approximately 143,000 Swiss francs in emergency funding to expand community awareness, household-level monitoring, and the distribution of medical and mosquito-prevention materials.[15]
Collaboration between WHO, IFRC, and local agencies was recognised as a strong example of coordinated public health response. The 2017 Peshawar dengue outbreak highlighted the importance of early surveillance, community participation, and cross-agency cooperation in controlling mosquito-borne diseases. Lessons learned from this outbreak continue to inform dengue preparedness and response strategies across Pakistan and other South Asian countries.[13]
The 2017 dengue outbreak in Peshawar, Khyber Pakhtunkhwa (KPK), Pakistan, was among the most severe public health crises in the region in recent years. It exposed significant gaps in urban infrastructure, community awareness, and governmental response capacity, while also providing valuable lessons for future vector-borne disease control.
Individual and Community Level
[edit]
Research on affected neighbourhoods showed that many people who live in impacted neighborhoods were found to be ignorant of how to prevent mosquito-borne illnesses[16]. Limited awareness reduced the chance of recognising early dengue symptoms, such as continuous fever and body pain, which often delayed treatment[17]. Research further documented the use of mosquito repellents, mosquito nets, and protective clothing during peak mosquito activity hours as frequent practices among residents with higher awareness levels [18]. Additional field surveys noted that regular cleaning of open containers, plant pots, and waste items reduced potential breeding sites around households, contributing to lower observed mosquito density in some communities[19].Residents need to actively participate in the community’s promotional activities to learn similiar basic measures for protecting themselves and minimize unnecessary transmission risks as much as possible.
Government and public-health response capacity
[edit]
Government documents show that the provincial administration established a Dengue Response Unit (DRU) to coordinate surveillance, laboratory diagnostics, vector control, and public communication[1]. Assessments of the outbreak response highlighted limitations such as restricted laboratory capacity and fragmented information systems[1]. The rapid increase in dengue cases placed pressure on health facilities, underscoring the significance of routine early warning mechanisms and stronger emergency management[1].
Media coverage had a significant influence on public perception during the outbreak[1]. Transparent reporting supported public trust, while inconsistent or inaccurate information occasionally contributed to confusion and reduced compliance. Analyses in public-health literature emphasised the importance of coordinated and consistent communication strategies to support community engagement during large outbreaks [1].
Environmental and multi-sectoral cooperation
[edit]
Environmental conditions were identified as major contributors to dengue transmission[16]. Studies associated climatic variation, rapid urbanisation, and ageing infrastructure with increased dengue incidence in the region[16]. Long term environmental management supported by monitoring of high-risk areas was considered essential for future prevention. Research also indicated that effective dengue control requires cooperation between public-health authorities and sectors such as water management, and urban planning [16].
Findings from the Peshawar outbreak have been used as reference points for improving vector-borne disease management across South Asia. Research outcomes contributed to discussions on strengthening surveillance systems, supporting community education, and improving collaboration across sectors.

References:
- ^ a b c d e f g h Saadia, H.; Nawaz, K.; Fatima, K.; Khan, S.; Sultana, K.; Haq, Iu; Ullah, A.; Ullah, J. (2025-03-13). “EPIDEMIOLOGICAL AND CLINICAL MANIFESTATIONS OF DENGUE IN DISTRICT PESHAWAR: A MULTI-CENTER STUDY”. Bulletin of Biological and Allied Sciences Research. 2025 (1): 93–93. doi:10.54112/bbasr.v2025i1.93. ISSN 2521-0092. Cite error: The named reference “:0” was defined multiple times with different content (see the help page).
- ^ “Peshawar Population 2025”. World Population Review. 2025-10-28. Retrieved 2025-10-31.
- ^ a b Urban Policy And Planning Unit. (2024). Peshawar City Master Plan, 2024-2044 – Volume One. Available at: https://urbanpolicyunit.gkp.pk/wp-content/uploads/2025/05/1.-Peshawar-City-Final-Master-Plan-2024-2044.pdf (Accessed: 27 October 2025).
- ^ a b c d Schaefer, Timothy J.; Panda, Prasan K.; Wolford, Robert W. (2025), “Dengue Fever”, StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 28613483, retrieved 2025-10-31
- ^ a b c d Khan, Najeeb Ullah; Danish, Lubna; Khan, Hydayat Ullah; Shah, Maryam; Ismail, Muhammad; Ali, Ijaz; Petruzziello, Arnolfo; Sabatino, Rocco; Guzzo, Annunziata; Botti, Gerardo; Iqbal, Aqib (2020). “Prevalence of dengue virus serotypes in the 2017 outbreak in Peshawar, KP, Pakistan”. Journal of Clinical Laboratory Analysis. 34 (9): e23371. doi:10.1002/jcla.23371. ISSN 1098-2825. PMC 7521314. PMID 32697383.
{{cite journal}}: CS1 maint: article number as page number (link) - ^ Shabbir, Waqas; Pilz, Juergen; Naeem, Amna (2020-06-25). “A spatial-temporal study for the spread of dengue depending on climate factors in Pakistan (2006-2017)”. BMC public health. 20 (1): 995. doi:10.1186/s12889-020-08846-8. ISSN 1471-2458. PMC 7318413. PMID 32586294.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ a b Agusto, F. B.; Khan, M. A. (2018). “Optimal control strategies for dengue transmission in pakistan”. Mathematical Biosciences. 305: 102–121. doi:10.1016/j.mbs.2018.09.007. ISSN 1879-3134. PMID 30218686.
- ^ a b c d e f g h i Abdullah, null; Ali, Sher; Salman, Muhammad; Din, Misbahud; Khan, Kachkol; Ahmad, Munib; Khan, Faisal Hayat; Arif, Muhammad (2019). “Dengue Outbreaks in Khyber Pakhtunkhwa (KPK), Pakistan in 2017: An Integrated Disease Surveillance and Response System (IDSRS)-Based Report”. Polish Journal of Microbiology. 68 (1): 115–119. doi:10.21307/pjm-2019-013. ISSN 2544-4646. PMC 7256837. PMID 31050259.
- ^ a b c d e f g h i “Pakistan: Dengue Outbreak Khyber Pakhtunkhwa (MDRPK014) DREF Operation Final Report – Pakistan | ReliefWeb”. reliefweb.int. 2018-03-22. Retrieved 2025-11-01.
- ^ a b c d e f g Haroon, Muhammad; Jan, Hasnain; Faisal, Shah; Ali, Nasir; Kamran, Muhammad; Ullah, Farhan (2019). “Dengue Outbreak in Peshawar: Clinical Features and Laboratory Markers of Dengue Virus Infection”. Journal of Infection and Public Health. 12 (2): 258–262. doi:10.1016/j.jiph.2018.10.138.
- ^ Minallah, Asim; Baig, A; Azam, N (2018-03-29). “Investigation of Dengue Fever Outbreak- District Peshawar, Pakistan, September 2017”. Iproceedings. 4 (1): e10630. doi:10.2196/10630. ISSN 2369-6893.
{{cite journal}}: CS1 maint: article number as page number (link) CS1 maint: unflagged free DOI (link) - ^ Shah, Fahad; Butt, Maryam; Iqbal, Attiya; Shah, Mian Naveed; Muhammad, Lal; Kousar, Nasim; Ulhaq, Farid (2018). “Institutional analysis of 2017 dengue outbreaks of Peshawar, Khyber Pakhtoonkhwa, Pakistan”. Journal of Entomology and Zoology Studies. 6 (2): 2475–2479. eISSN 2320-7078 – via Entomol Journal.
- ^ a b c d e f “Outbreak update – Dengue in Pakistan, 26 October 2017”. World Health Organization – Regional Office for the Eastern Mediterranean. 26 October 2017. Retrieved 2 November 2025.
- ^ a b “Khyber Pakhtunkhwa Health Department Dengue Situation Report 2017”. Government of Khyber Pakhtunkhwa. Retrieved 2 November 2025.
- ^ a b “Emergency Plan of Action Final Report – Pakistan: Dengue Outbreak”. International Federation of Red Cross and Red Crescent Societies. 2018. Retrieved 2 November 2025.
- ^ a b c d Shabbir, Waqas; Pilz, Juergen; Naeem, Amna (2020-06-25). “A spatial-temporal study for the spread of dengue depending on climate factors in Pakistan (2006–2017)”. BMC Public Health. 20 (1): 995. doi:10.1186/s12889-020-08846-8. ISSN 1471-2458. PMC 7318413. PMID 32586294.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ Aminullah -; Hassan, Soaib Ali; Khail, Ashfaq Ahmed Khawaja; Waris, Abdul; Alam, Gul; Marwat, Salahuddin Khan (2017-09-30). “ASSESSMENT OF KNOWLEDGE, ATTITUDE AND PRACTICES REGARDING DENGUE FEVER AMONG ADULT POPULATION OF DISTRICT DIR LOWER, KHYBER PAKHTUNKHWA, PAKISTAN”. Pakistan Journal of Public Health. 7 (2): 71–74. doi:10.32413/pjph.v7i2.35. ISSN 2226-7018.
- ^ Khan, Jehangir; Adil, Muhammad; Wang, Gang; Tsheten, Tsheten; Zhang, Dongjing; Pan, Wenjie; Khan, Munir Ahmad; Rehman, Inayat ur; Zheng, Xiaoying; Wu, Zhongdao; Wu, Yu (2022-07-29). “A cross-sectional study to assess the epidemiological situation and associated risk factors of dengue fever; knowledge, attitudes, and practices about dengue prevention in Khyber Pakhtunkhwa Province, Pakistan”. Frontiers in Public Health. 10. doi:10.3389/fpubh.2022.923277. ISSN 2296-2565.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ Mukhtar, Muhammad Uzair; Han, Qian; Liao, Chenhong; Haq, Fatima; Arslan, Ali; Bhatti, Adil (2018-06-28). “Seasonal Distribution and Container Preference Ratio of the Dengue Fever Vector (Aedes aegypti, Diptera: Culicidae) in Rawalpindi, Pakistan”. Journal of Medical Entomology. 55 (4): 1011–1015. doi:10.1093/jme/tjy010. ISSN 1938-2928. PMID 29462424.